
Walk through an average South African hospital, and you’ll see crowded waiting rooms full of unstable patients. Meet the diverse patients hailing from the largest cities and the smallest villages. Admire the nurses who work tirelessly to provide care despite staffing shortages and crumbling hospital infrastructure.
Drive ten minutes through the city and arrive at a state-of-the-art hospital. Now, you’ll observe the overwhelmingly white patients who fly from around the world to reap the benefits of their privilege. The benefits include accomplished staff, brand-new machines, and immediate care. Such is the state of inequality that continues to plague South Africa post-apartheid.
“South Africa was wounded by its history of apartheid, leaving scars of financial inequality that bleed the health disparities we view today.”
This summer, I explored healthcare in South Africa on a Northeastern University Dialogue of Civilizations. I traveled alongside a group of 20 students, primarily health science majors, and we were given unrestricted access to many public and private hospitals in South Africa. South Africa provides universal healthcare to its citizens, but the difference in care between public hospitals and the private hospitals used by the wealthy is stark. In comparison, America is primarily driven through a private healthcare system, with some governmental health coverage provided through Medicare and Medicaid. It provides a consistent standard of care — but only to those who are insured. Both health systems have their own positive features, alongside their weaknesses.
Public hospitals: Staffing shortages and wait times
The South African universal healthcare system is divided into three major levels: national, provincial, and local. Sue Armstrong, a professor at the University of the Witwatersrand, explained to our class that the national level creates healthcare policies but can do little to enforce them upon provinces. Each province manages its hospitals and its healthcare budget depending on the needs of its people. Local clinics function as ground-level providers that make healthcare accessible to all in South Africa. They exist in the highest number of all the three levels of healthcare.
The local clinics are spread throughout the many rural areas and developing townships of South Africa in order to provide medical care to those who aren’t fortunate enough to live close to a major hospital. Our class was given a tour of one of these clinics at Chiawelo Community Health Center. What immediately stood out was the lack of doctors. The clinic focused on primary care and was primarily nurse-run alongside a few physician assistants. During our tour, a physician assistant explained to us that — unlike in America — in South Africa, many nurses are certified to prescribe medicine. This was one of many healthcare policies the South African government has put in place to subdue the shortage of doctors.
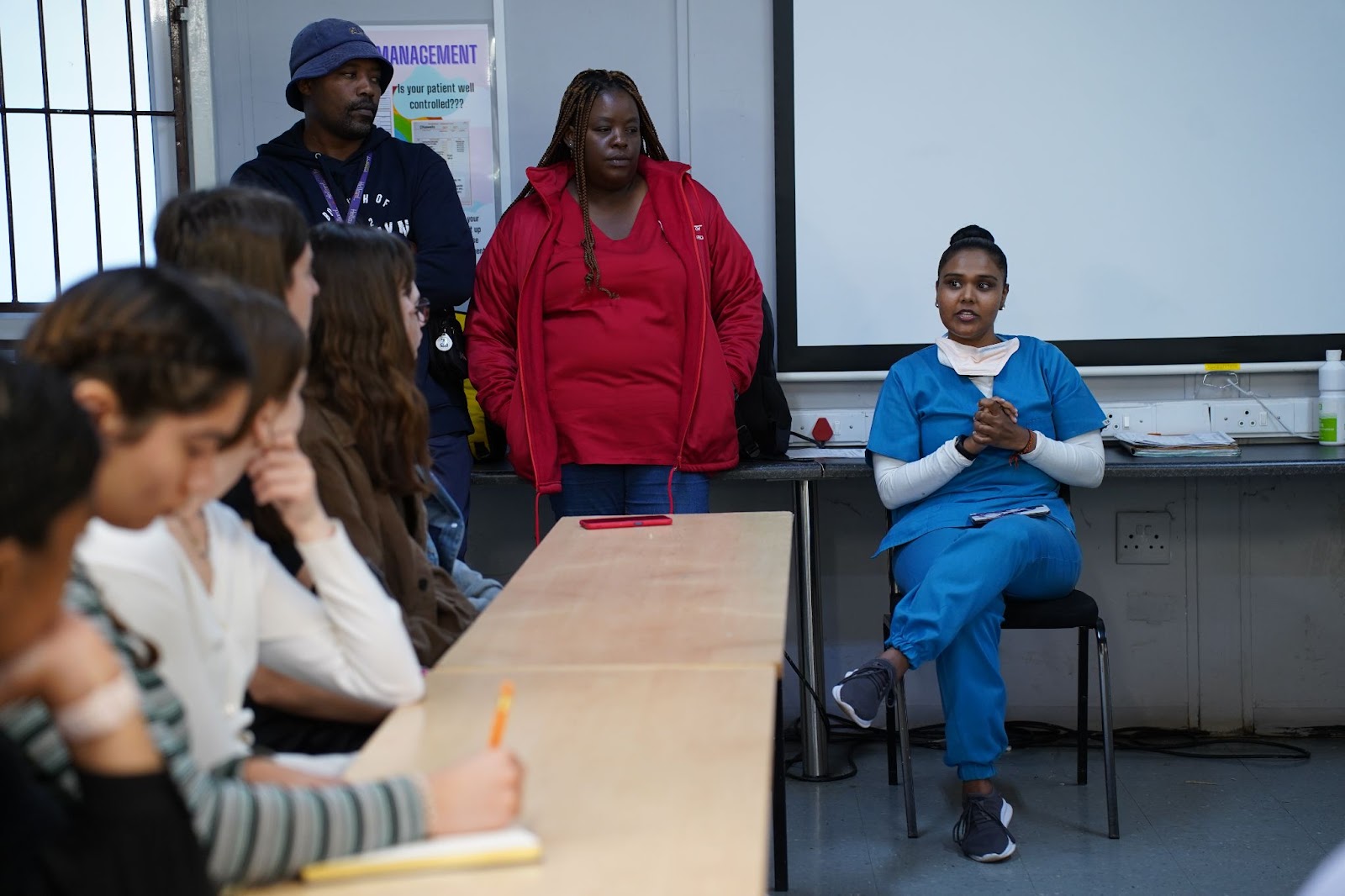
Inside the Chiawelo Community Health Center, near Johannesburg. Photo by Anna Deng, Designer and Videographer for Northeastern University
On a visit to the Charlotte Maxeke Johannesburg Academic Hospital a few days later, our class was able to observe the emergency department, operating rooms, and even medical imaging rooms. A group of students and I even got the opportunity to put on scrubs, observe two operating rooms, and interview surgeons. When asked about any problems they’ve directly noticed in the healthcare system, the surgeons emphasized a problem with waiting times. They explained that non-life-threatening surgeries have extreme wait times and are difficult to obtain without seeking private hospitals.

The Charlotte Maxeke Johannesburg Academic Hospital, associated with the University of the Witwatersrand, in Johannesburg. Photo by Anna Deng, Designer and Videographer for Northeastern University
This issue of waiting times was evident among the other parts of the hospital we visited, perhaps as a result of staffing shortages. The emergency room was very crowded and it was clear that patients with severe, debilitating injuries were not being seen at a rate comparable to the U.S. Apart from the problems, the surgeons emphasized that the beauty of their healthcare system is that everyone receives some form of value and care at little to no cost.
Private hospitals: Same country, a different world
One week passed after our visit to the Charlotte Maxeke Johannesburg Academic Hospital. We traveled from Johannesburg to the beautiful city of Cape Town. Surrounded by the sea and coastal beaches, the vacation town had a calmer atmosphere than the bustling and industrialized Johannesburg. Instead of visiting a public hospital, our class explored the Life Vincent Pallotti Private Hospital and had a very different experience.

The view of Table Mountain in Cape Town. Photo by Anna Deng, Designer and Videographer for Northeastern University
This hospital was fully staffed, clean, and according to the employees, the oncology center contained some of the “best radiation equipment in Africa.” I was taken into a chemotherapy center, and the nurses explained to me that wealthy people from around the world would travel to access the excellent facilities at the hospital. Furthermore, I noticed that it was much less busy than the public hospitals we had visited, and the wait times seemed insignificant.
“Visiting South Africa allowed me to better understand global health systems and how they can play a part in improving American health policies.”
Our group noticed that the majority of the patients in the hospital were white, which stood out considering that only 8% of South Africa’s population is white. Unsurprisingly, when we asked our hospital guide about this, they dismissed it immediately without a thoughtful response.
Exploring this hospital helped us to better understand the idea of disparity. According to the CDC, health disparities “are preventable differences in the burden of disease, injury, violence, or opportunities to achieve optimal health that are experienced by socially disadvantaged populations.”
Our class visited the Apartheid Museum, alongside the Mandela House, and these experiences gave us a glimpse of some of the ugly injustices that took place in such a beautiful nation. South Africa’s massive health disparity can be better understood through its history of Apartheid. Apartheid was the policy of racial apartness, which segregated South Africa through its schools, housing, and hospitals until 1994. Although the physical policy of Apartheid has been done away with, South Africa was wounded, leaving scars of financial inequality that bleed the health disparities we view today.

Visiting the Apartheid Museum in Johannesburg. Photo by Anna Deng, Designer and Videographer for Northeastern University
How Does the US Compare?
Extreme healthcare inequality is not isolated to South Africa. Although America is home to some of the greatest research and medical facilities in the world, 27.5 million Americans are uninsured and cannot afford to access them. Both South Africa and the U.S.’s healthcare systems have successful aspects alongside their flaws. As an American public health student, I have seen many interesting South African innovations that I wish America would adopt and vice versa.
The beauty of the American system is that people with private and governmental insurance are able to walk into the same hospital and receive a similar standard of care. South Africa’s system creates two different worlds. By having separate standards and hospitals for the public and private systems, South Africa creates financial segregation and causes the poor to receive a lower level of care than the rich. But South Africa’s ability to make healthcare accessible to all is admirable. The country does what America fails to and ensures that all of its citizens receive some form of healthcare.
To achieve universal healthcare is very difficult, however, and something more feasible that America can adopt from South Africa is their larger presence of nurses in healthcare. Professional nurses can prescribe medicine in South Africa, which allows far more people who cannot reach doctors to access healthcare. This concept could be applied in America to lower the costs of healthcare as individuals could see nurses instead of doctors for certain medications and potentially pay less for the same appointments.
South Africa has also begun using community-oriented healthcare models that utilize community health workers who physically enter communities and perform checkups in people’s homes, providing high population access and satisfaction. If these models are carried out at the same standard of care as our private system, they can be applied to lower-income communities in the U.S. to provide low-cost healthcare to a large scale of people.
Healthcare access is an extremely complex and expensive issue that does not have a clear solution in America or South Africa. However, both nations have certain aspects that work within their healthcare systems, and both are able to learn from each other. Visiting South Africa allowed me to better understand global health systems and how they can play a part in improving American health policies. I dream that a day will come when the governments of South Africa and America will be able to provide quality healthcare to their citizens as a basic human right. I imagine that one day I will visit South Africa again to see a high-quality universal healthcare system, and return to America to find a healthcare system that doesn’t exclude those with less.
